Background
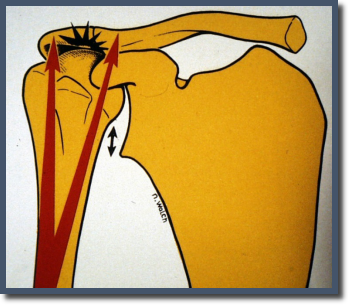
Most rotator cuff tears in young active patients are treated surgically, with good to excellent results in the vast majority of patients. However, tears that go undiagnosed for a prolonged period of time gradually become more and more retracted, scarring in place in a very retracted position. The associated muscles often atrophy. Patients with this problem usually present with a combination of pain and weakness. Without a functioning rotator cuff, the deltoid lacks a fulcrum to pull against. When the deltoid contracts in an attempt to lift the arm, the humerus instead elevates, running into the upper shoulder blade (acromion). This creates pain and an inability to lift the arm effectively.
In older patients, a good solution to this problem is reverse shoulder arthroplasty, or RSA. This procedure changes the mechanics of the shoulder, so that the rotator cuff is no longer needed for elevating the arm. The deltoid can function more independently and lift the arm again. Unfortunately these devices were not meant for the heavy demands younger people typically place on them. Therefore, RSA is not a great option in patients under 50 or those who place high demands on their shoulder.
Younger patients with very symptomatic irreparable rotator cuff tears can be treated with tendon transfers, to reroute another tendon (such as the latissimus dorsi or the pectoralis major) to take the place of the functioning rotator cuff. However, results from tendon transfers vary widely, and rehabilitation often very lengthy and complicated.
The Rational for Superior Capsular Reconsctruction (SCR)
Because these younger patients had no great option for treatment, surgeons began searching for an alternative. Japanese surgeon Teruhisa Mihata developed the superior capsular reconstruction (SCR) in 2007. Like the RSA, this procedure changed the mechanics of the shoulder so the deltoid could lift the arm irrespective of the absent rotator cuff. However, unlike the RSA, SCR does not replace any part of the joint. It can also be done arthroscopically. Therefore pain relief is more immediate, recovery is faster, and ultimate activities are more unrestricted, since there are no joint replacement parts to wear out. In addition, this procedure does not burn any bridges. In other words, any other shoulder procedure could still be performed in the future (including another SCR!). This makes SCR a very attractive option for younger patients with irreparable rotator cuff tears, or older patients who otherwise don’t need a joint replacement.
Procedure
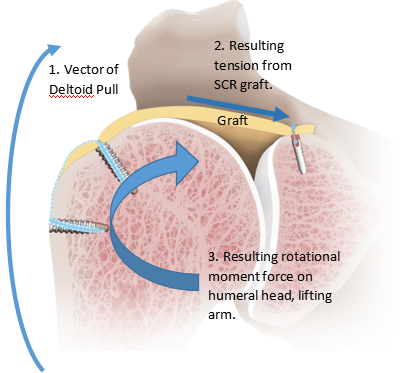
In an SCR, allograft tissue (usually cadaveric dermis) is used to attach the upper humerus (arm bone) to the upper shoulder socket. This is a technically straightforward and relatively fast procedure. It is done as an outpatient like most other arthroscopic shoulder procedures.
Rehabilitation and Recovery
The process of physical therapy and rehabilitation is similar after SCR as compared to traditional rotator cuff repair. Time is needed for the allograft to begin to heal to the two bony attachment sites. However, once healing has progressed well, the strengthening phase of the rehab often goes faster, because there is no need to strengthen the small rotator cuff muscles. Strengthening focuses instead on the deltoid, which tends to rehab faster given its large size and bulk.
For more information about our services or to schedule an appointment, call us at / / or click here to request an appointment online. We’ll respond to you as soon as possible.