Natalie Bain, MS4 Brian Gilmer, MD, Timothy Crall, MD
Case Example
A 45-year-old male presents with shoulder pain for the last few months. It started when he was chopping wood and swinging the ax. He felt a pain like being “punched on the inside of his shoulder.” Afterward, it felt like his arm was going to fall off. He frequently chops wood and was noticing an increasing dead-arm sensation. Ibuprofen has helped the pain slightly.
Introduction
Superior labrum anterior-to-posterior (SLAP) tears were first described in 1985 from findings on arthroscopic surgeries [1]. SLAP tears occur when the gasket-like cartilage of the labrum is torn in an anterior to posterior direction. They are frequently asymptomatic but may be present in up to 26% of shoulder arthroscopies [2]. Famous as a baseball injury, SLAP tears typically occur in patients who engage in frequent overhead motions. There is much debate surrounding the management of SLAP tears, but the level of patient demand on the shoulder should direct intervention. Concomitant injuries are very common in the setting of SLAP tears and should be considered in developing a treatment plan.
Anatomy
The shoulder is a ball-and-socket joint maximized for range of motion. Important structures for SLAP tears include the humeral head (ball), glenoid (socket), labrum (cushion over the glenoid), and biceps tendon (Image 1). SLAP tears involve the tendon of the long head of the biceps and the labrum. The biceps tendon courses over the humeral head and attaches to the labrum. Under tension, it can forcefully pull the labrum off the glenoid. The resulting injury may go unnoticed, may cause significant pain or decreased function, or may even be a beneficial adaptation [3].
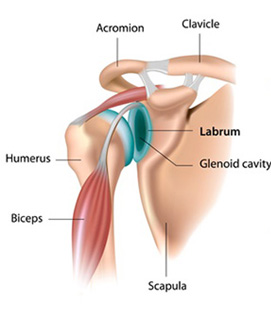 Image 1. Normal anatomy of the shoulder ball-in-socket joint showing the long head of the biceps tendon attaching to the gasket-like cartilage of the labrum [4].
Image 1. Normal anatomy of the shoulder ball-in-socket joint showing the long head of the biceps tendon attaching to the gasket-like cartilage of the labrum [4].
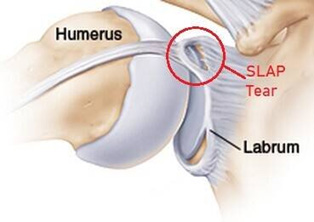 Image 2. SLAP tear showing biceps tendon tension tearing the labrum off the glenoid [5].
Image 2. SLAP tear showing biceps tendon tension tearing the labrum off the glenoid [5].
History
SLAP tears may result from chronic strain or acute injury [3].
Chronic strain is usually caused by frequent overhead motions that damage the labrum over time. Patients may notice decreased strength in throwing or decreased range of motion. Clicking or catching may also be felt when the arm is abducted and externally rotated. Posterior or deep pain is common for chronic labral damage.
Acute labral injury can be the result of traction, trauma, or quick jerking motions. Traction includes movements such as lifting heavy objects, while falling on an outstretch arm should raise suspicion for traumatic labral injury. Anterior or deep shoulder pain is frequently described by patients with an acute labral injury.
Physical Exam
A complete evaluation of the shoulder should be performed due to the high likelihood of concomitant shoulder injuries. SLAP tear-specific exam maneuvers include many of the same maneuvers that evaluate for biceps tendon pathology or shoulder instability. The history, physical exam, imaging, and arthroscopy all contribute to the diagnosis.
- Belly Press Test: Best test to rule in SLAP tears (85% specificity) [3], although most commonly used for subscapularis examination. Patient places hand on belly with elbow at 90 degrees. Pressure is applied with palm against belly to bring the elbow out in front of the plane of the abdomen.
- Anterior Glide Test: This is also a good exam maneuver for ruling in SLAP tears (82% specificity) [3]. Patient lies supine while examiner places an axial load on the joint line of the shoulder as shown in Image 3 [4].
 Image 3 [6]. Anterior glide test.
Image 3 [6]. Anterior glide test.
- Modified dynamic labral shear test: Best test to help rule out other shoulder pathologies (80% sensitivity) [3]. Pain or catching when pressure is applied through the shoulder joint as the arm is adducted from 120 degrees to 60 degrees indicates a positive test (Image 4).
 Image 4 [7]. Modified dynamic labral shear test.
Image 4 [7]. Modified dynamic labral shear test.
- Supine flexion resistance test: Helpful to rule out other shoulder pathologies (80% sensitivity) [3]. Deep pain elicited inside the shoulder joint or at the dorsal aspect of the shoulder when downward pressure is applied to a fully elevated arm is a positive exam finding (Image 5).
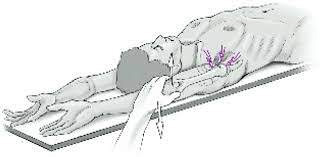 Image 5 [8]. Superior flexion resistance test.
Image 5 [8]. Superior flexion resistance test.
Imaging
Imaging is an important part of the evaluation of acute and chronic shoulder complaints.
Plain Films: Three different views of the shoulder are typically used to evaluate shoulder pathology: anterior-posterior view (Grashey view), axillary lateral view, and the outlet view. In the setting of SLAP tears, plain films are helping for assessing for any other shoulder pathology thay may be present.
 Image 6 [9]. AP view of the shoulder (“Grashey” view).
Image 6 [9]. AP view of the shoulder (“Grashey” view).
 Image 7 [10]. Axillary lateral view of the shoulder.
Image 7 [10]. Axillary lateral view of the shoulder.
 Image 8 [11]. Shoulder outlet view.
Image 8 [11]. Shoulder outlet view.
MRI: Not recommended in older patients solely for identifying SLAP lesions. SLAP lesions in older patients are largely asymptomatic and MRI can lead to overdiagnosis. MRI is useful in younger patients (<35 years old) and can be made even more sensitive with the use of contrast (MR arthrogram).
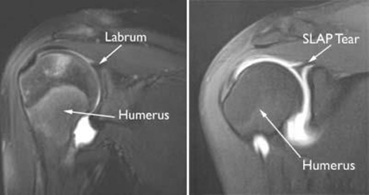 Image 9 [12]. The labrum is seen as a dark triangle in a normal shoulder. SLAP tears are evidenced by bright signaling where there would otherwise be a lack of signal.
Image 9 [12]. The labrum is seen as a dark triangle in a normal shoulder. SLAP tears are evidenced by bright signaling where there would otherwise be a lack of signal.
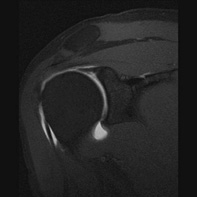 Image 10 [12]. SLAP tear indicated by white signal in what would normally be a pure black triangle of the labrum.
Image 10 [12]. SLAP tear indicated by white signal in what would normally be a pure black triangle of the labrum.
Treatment
Non-operative management: Helpful to alleviate pain, regain functionality, and avoid surgical management which portends a long recovery period and unpredictable outcomes.
- Reduce aggravating actions
- Acetaminophen and NSAIDs
- Physical therapy is encouraged to strengthen surrounding muscles, which may help remove pressure from the site of injury. Therapy will also help with range of motion.
Operative management: Guided by the eight classifications for SLAP tears as determined by history and arthroscopic findings, operative management is reserved for patients who fail non-operative treatment and have persistent pain/loss of function that impacts desired activates or activities of daily living [3].
- Type I: Chronic type injury with fraying around the labrum.
- Surgery: Arthroscopic debridement.
- Type II: Acute type injury with tearing of the labrum and long head of the biceps and avulsion of the labrum off the glenoid.
- Surgery: Repair of SLAP lesion, biceps tendon release (tenotomy), or biceps tendon release with reattachment (tenodesis).
- Type III: Very rare, bucket-handle type injury where the labrum is torn off the glenoid but the long head of the biceps is intact.
- Surgery: Repair of SLAP tear or removal of avulsed cartilage.
- Type IV: Common in the setting of shoulder instability. Considered a Type III injury plus tearing of the long head of the biceps.
- Surgery: SLAP repair or release if <50% of biceps tendon damaged, biceps tenotomy/tenodesis if >50% biceps tendon involved.
- Type V: A Type II SLAP tear with additional anterior shoulder instability.
- Surgery: SLAP lesion repair.
- Type VI: Findings of superior labral flaps with no injury to the long head of the biceps.
- Surgery: SLAP repair or resection.
- Type VII: Type II SLAP tear with inferior glenohumeral ligament instability.
- Surgery: Repair of anterior labrum with SLAP repair.
- Type VIII: Type II SLAP tear with additional cartilage injury.
- Surgery: debridement, SLAP repair or biceps tenotomy/tenodesis.
References
- Andrews, JR, Carson, WG, McLeod, WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med. 1985;13:337-341.
- T.K. Kim, W.S. Queale, A.J. Cosgarea, E.G. McFarland. Clinical features of the different types of SLAP lesions: an analysis of one hundred and thirty-nine cases. J Bone Joint Surg Am, 85 (2003), pp. 66-71.
- Varacallo M, Tapscott DC, Mair SD. Superior Labrum Anterior Posterior (SLAP) Lesions. [Updated 2020 Mar 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www-ncbi-nlm-nih-gov.unr.idm.oclc.org/books/NBK538284/
- https://www.shoulder-pain-explained.com/images/xSLAP-tear-shoulder.jpg.pagespeed.ic.wllN81E3XW.jpg
- https://www.rebuildphysiotherapy.com/post/shoulder-labrum-tear
- Ireland, Mary Lloyd, and John Hatzenbuehler. “Superior Labrum Anterior Posterior (SLAP) Tears.” UpToDate, 25 Oct. 2018, www.uptodate.com/contents/superior-labrum-anterior-posterior-slap-tears?search=slap+tear.
- Myer CA, Hegedus EJ, Tarara DT, et alA user's guide to performance of the best shoulder physical examination testsBritish Journal of Sports Medicine 2013;47:903-907.
- Ebinger N, Magosch P, Lichtenberg S, Habermeyer P. A new SLAP test: the supine flexion resistance test. Arthroscopy. 2008;24(5):500-505. doi:10.1016/j.arthro.2007.11.017
- https://radiopaedia.org/cases/grashey-view-ap-oblique-shoulder-radiograph
- https://www.aoaortho.com/axillary-lateral-view/
- https://radiopaedia.org/articles/shoulder-outlet-view?lang=us
- https://orthoinfo.aaos.org/en/diseases--conditions/slap-tears/
- Gaillard, Frank. “Superior Labral Anterior Posterior Tear | Radiology Reference Article | Radiopaedia.Org.” Radiopaedia, radiopaedia.org/articles/superior-labral-anterior-posterior-tear?lang=us. Accessed 12 Sept. 2020
For more information about our services or to schedule an appointment, call us at / / or click here to request an appointment online. We’ll respond to you as soon as possible.