
















Scapulothoracic Dissociation
Steven Kim, MS4, Dr. Gilmer, MD
Scapulothoracic dissociation is a rare and potentially life-threatening injury with a mortality rate of approximately 11%. Often associated with polytrauma, scapulothoracic dissociation has the potential to be overlooked in the acute setting. This can lead to delayed diagnosis and treatment of this potentially debilitating injury. Therefore, awareness of this condition should be high in patients with high-energy shoulder girdle injuries.
Scapulothoracic Dissociation
Case
A 55-year-old male presents to the trauma bay for evaluation after a dirt bike accident. The patient was traveling at 20 mph when he hit another dirt bike head on (also traveling at 20 mph). Patient was in full protective gear including a helmet, but sustained blunt trauma to the left shoulder and left arm. The patient states that his left shoulder feels crunchy and he is having tingling and decreased motor function in his hands and fingers.
Introduction
Scapulothoracic dissociation is a rare and potentially life-threatening injury with a mortality rate of approximately 11% [1]. Often associated with polytrauma, scapulothoracic dissociation has the potential to be overlooked in the acute setting. This can lead to delayed diagnosis and treatment of this potentially devastating injury [2]. Therefore, awareness of this condition should be high in patients with high-energy shoulder girdle injuries.
Anatomy
The shoulder is formed by three bones: the clavicle, scapula, and proximal humerus. The scapula is a flat triangular bone located at the back of the trunk and resides over the posterior surface of ribs two to seven. The scapula, along with the clavicle and the manubrium of the sternum, make up the shoulder girdle which connects the upper limb of the appendicular skeleton to the axial skeleton [3].
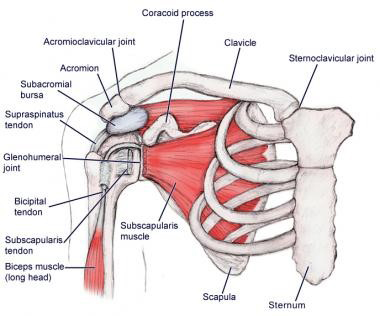
The scapula provides a point of attachment for a number of muscles that make up the arm and shoulder. It articulates with the humerus (forming the glenohumeral joint), the clavicle (forming the acromioclavicular joint), and the sternum (forming the sternoclavicular joint). The medial aspect of the scapula is connected to the thorax and vertebral column by muscles, allowing the scapula to move freely across the posterior thoracic wall via the scapulothoracic joint [3]. This provides a wide range of movement and mobility for the upper limb compared to the lower limb.
Scapulothoracic dissociation
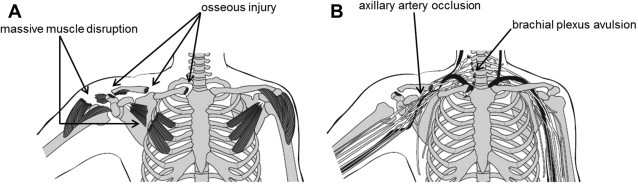
Scapulothoracic dissociation refers to a spectrum of musculoskeletal, vascular, and neurologic abnormalities that includes a laterally displaced scapula with an ipsilateral clavicular fracture, AC joint separation or sternoclavicular joint disruption [1]. Concomitant injuries to subclavian or axillary vessels and the brachial plexus can occur. Originally described with intact overlying skin, open injuries have also been reported. A closed scapulothoracic dissociation with neurovascular injury is called a closed forequarter amputation [4].
Mechanism
Scapulothoracic dissociation results from high-energy traction injuries, typically from a motorcycle or motor vehicle accident. is usually caused by a severe direct force applied over the shoulder accompanied by a fixed upper extremity (eg. secondary to gripping a motorcycle handle or steering wheel) [2]. Patients have an increased risk of polytrauma, including severe life-threatening injuries to other body parts and ipsilateral upper extremity.
History and Physical Exam
Presumptive diagnosis of is based on a history of high-energy trauma and presence of massive soft tissue swelling over shoulder girdle [4]. If the patient’s clinical situation allows, a thorough physical exam including a neurological exam should be obtained [2]. Inspection will show significant swelling and bruising around shoulder region due to variable combinations of edema, hematoma, and muscle tears [2, 4]. Vascular injury has been reported in 64-100% of patients with scapulothoracic dissociation and is usually due to thrombosis or compression of subclavian or axillary vessels [5]. Physical exam may show decreased or absent pulses, pallor, and coolness of affected extremity. A thorough neurological exam should be performed for determination of the presence and extent of neurologic injury. Neurological status is critical part of exam as it is a main determinant of functional outcome [4].
Imaging
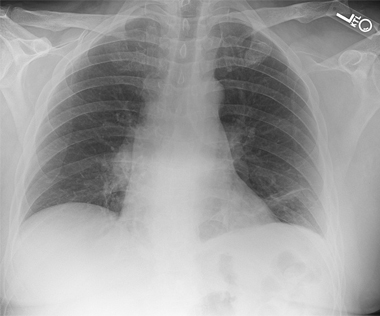
AP chest radiography should be performed as part of initial trauma series. On a nonrotated chest radiograph, assessment of lateral scapular displacement can be performed by measuring distance between a midline thoracic spinous process and the medial borders of the scapula on both the injured and uninjured sides. A difference > 1 cm is diagnostic of scapulothoracic dissociation [1, 5]. Orthogonal radiographs of any suspected upper extremity fracture or dislocation should also be obtained. Immediate Vascular imaging with CT angiography is recommended in patients with suspected scapulothoracic dissociation [2]. CT myelography, MRI, or EMG studies can be used for evaluation of brachial plexus injuries. Nerve studies are usually reserved for at least 3 weeks after injury to assess degree of recovery, if any.
Management
Because of the complexity of concomitant injuries, a multidisciplinary approach to management of scapulothoracic dissociation is necessary. Initial treatment of patients follows the advanced trauma life support protocol. Airway, breathing, and circulation should be assessed and treated appropriately. If vascular integrity of the involved upper extremity is in question, an emergency arteriogram is performed, followed by surgical repair, if necessary [2]. Reduction and stabilization of ipsilateral upper limb fractures as well as any shoulder joint disruptions are indicated, although there is little evidence the guide the timing of orthopedic interventions [6]. Immediate orthopedic intervention may be necessary when there is a progressive neurologic deficit or need for stabilization after vascular repair [1]. Surgical management of brachial plexus injuries may include nerve grafting or above-elbow amputation. Above-elbow amputation is usually reserved for patients with complete brachial plexus injuries due to presence of flail upper limb (complete loss of sensory and motor function) [2].

Prognosis
Vascular injury has been reported in 64-100% of patients with STDs. However, due to presence of extensive shoulder girdle collateral arteries, life-threatening hemorrhage and limb ischemia are relatively uncommon and overall outcomes related to vascular injury are good [2]. Neurologic injury is the main determinant of functional outcome after STDs and therefore neurologic assessment is critical. Approximately 52% of patients with STD will have a flail nonfunctional upper extremity [1].
References
1. Kani KK, Chew FS. Scapulothoracic dissociation. British Institute of Radiology. 2019
2. Choo AM, Schottel PC, Burgess AR. Scapulothoracic dissociation: evaluation and management. J Am Acad Orthop Surg. 2017; 25: 39-47.
3. KenHub. Anatomy of scapula. 2019. www.kenhub.com/en/library/anatomy/scapula/. Accessed July 28, 2019.
4. Rockwood CA, Matsen FA, Wirth MA, Lippitt SB. Lateral dislocation of the scapula. The Shoulder. 2014, pp. 364-366.
5. Zelle BA, Pape H-C, Gerich TG, Garapati R, Ceylan B, Krettek C. Functional outcome following scapulothoracic dissociation. The Journal of Bone and Joint Surgery-American Volume. 2004; 86A: 2-8.
6. Flanagin BA, Leslie MP, Scapulothoracic dissociation. Orthop Clin North Am. 2013; 44:1-7.



